Breast Implant Removal & Exchange
Breast implant removal, also known as explant surgery, is a procedure performed to remove silicone or saline breast implants that are no longer wanted, no longer suitable, or are causing cosmetic or medical concerns.
In Leeds, breast implant removal is performed by Consultant Oncoplastic Breast Surgeon Mr Philip Turton, who specialises in explantation, capsulectomy and breast reshaping procedures to help patients achieve the safest and most natural outcome possible.
The procedure may be performed on its own or combined with a breast uplift (mastopexy) to restore shape and nipple position following implant removal.


Why Breast Implant Removal
Women choose breast implant removal for a variety of personal, cosmetic and medical reasons. Some no longer wish to have implants, while others experience implant-related complications or changes in breast shape over time.
Common reasons include capsular contracture, implant rupture, concerns regarding breast implant illness (BII), ageing-related breast changes, lifestyle preferences, or a desire for a more natural appearance.
For many patients, implant removal is combined with breast uplift surgery to address stretched skin, breast droop and loss of breast shape that can occur after explantation.
Reasons for choosing Breast Implant Removal
Breast implant removal is a highly individual decision. Patients may seek treatment because of physical symptoms, changes in appearance, or a desire to return to a more natural breast shape.
Aesthetic Concerns
- Preference for a smaller or more natural breast size
- Breast sagging following implants
- Changes in breast shape due to ageing
- Implants no longer suit lifestyle or appearance goals
- Concerns about asymmetry or implant position
Physical Concerns
- Capsular contracture causing hardness or discomfort
- Implant rupture or suspected leakage
- Chronic pain or recurrent seromas
- Concerns regarding implant-related symptoms
- Ongoing implant monitoring or replacement requirements
Emotional & Social Impacts
- Desire to feel more comfortable without implants
- Anxiety about implant complications
- Reduced confidence due to breast changes
- Preference to avoid future implant surgery
- Seeking peace of mind following implant concerns
The Procedure
Breast implant removal is tailored to the reason for explantation and the condition of the implants and surrounding tissue. Depending on the findings, surgery may involve simple implant removal, removal of scar capsule tissue (capsulectomy), or simultaneous breast uplift surgery to improve breast shape after explantation.
01
General anaesthetic administered.
02
Existing implant incision reopened where possible – removal of implants.
03
Partial or total capsulectomy performed if indicated – capsule tissue sent for histopathology where appropriate.
04
Breast uplift performed if planned – wound closure and post-operative monitoring.
DURATION:
Typically 1–3 hours depending on whether capsulectomy and mastopexy are required. En-bloc capsulectomy procedures can take significantly longer.



Safety and Recovery for Breast Implant Removal
Breast implant removal is generally considered safe when performed by an experienced specialist breast surgeon. The complexity of surgery varies significantly depending on whether capsule removal is required and whether implants are positioned above or below the chest muscle.
Potential risks include:
- Haematoma (blood collection)
- Seroma (fluid collection)
- Infection
- Cosmetic dissatisfaction
- Residual breast sagging
- Scarring
- Temporary discomfort or soreness
- Risks associated with extensive capsulectomy procedures
Patients considering total capsulectomy should understand that complete capsule removal is not always appropriate or safe, particularly where the capsule is adherent to ribs, muscles or other important structures.
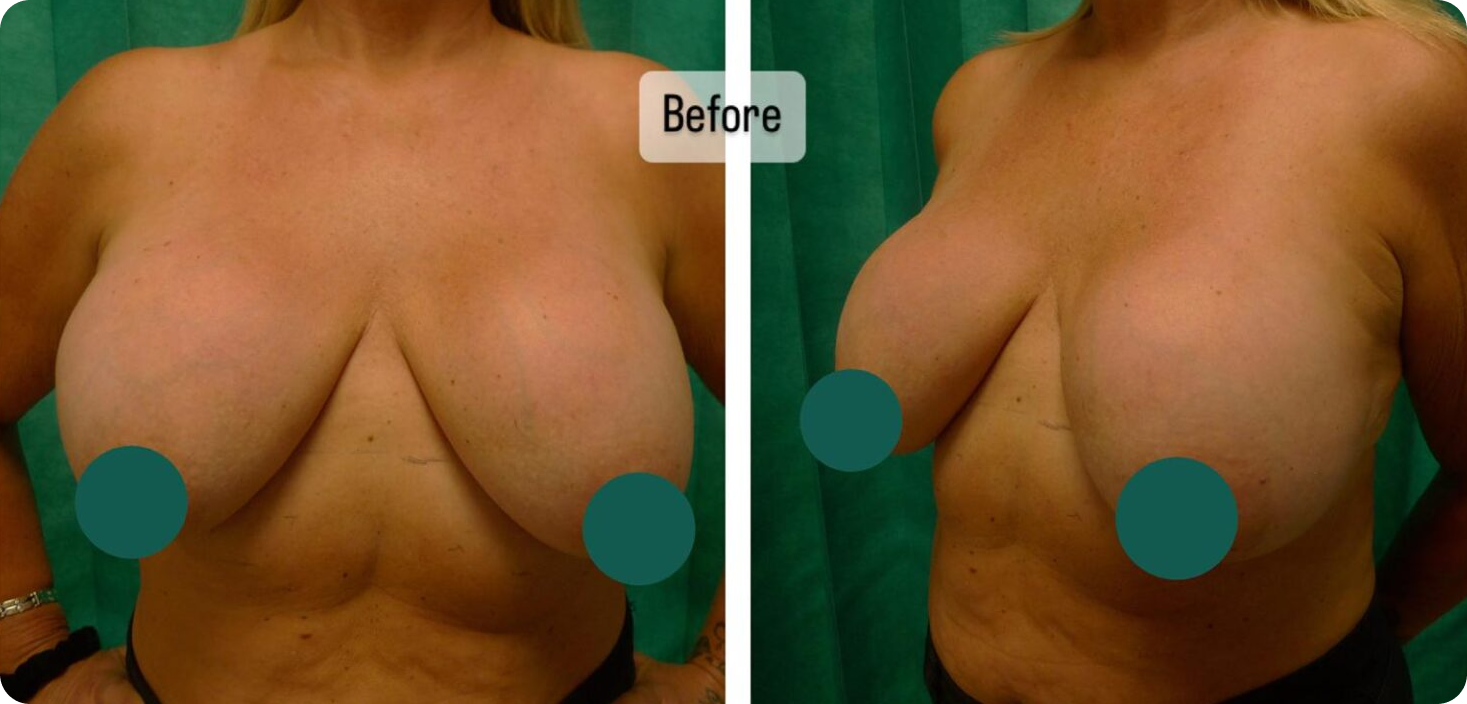
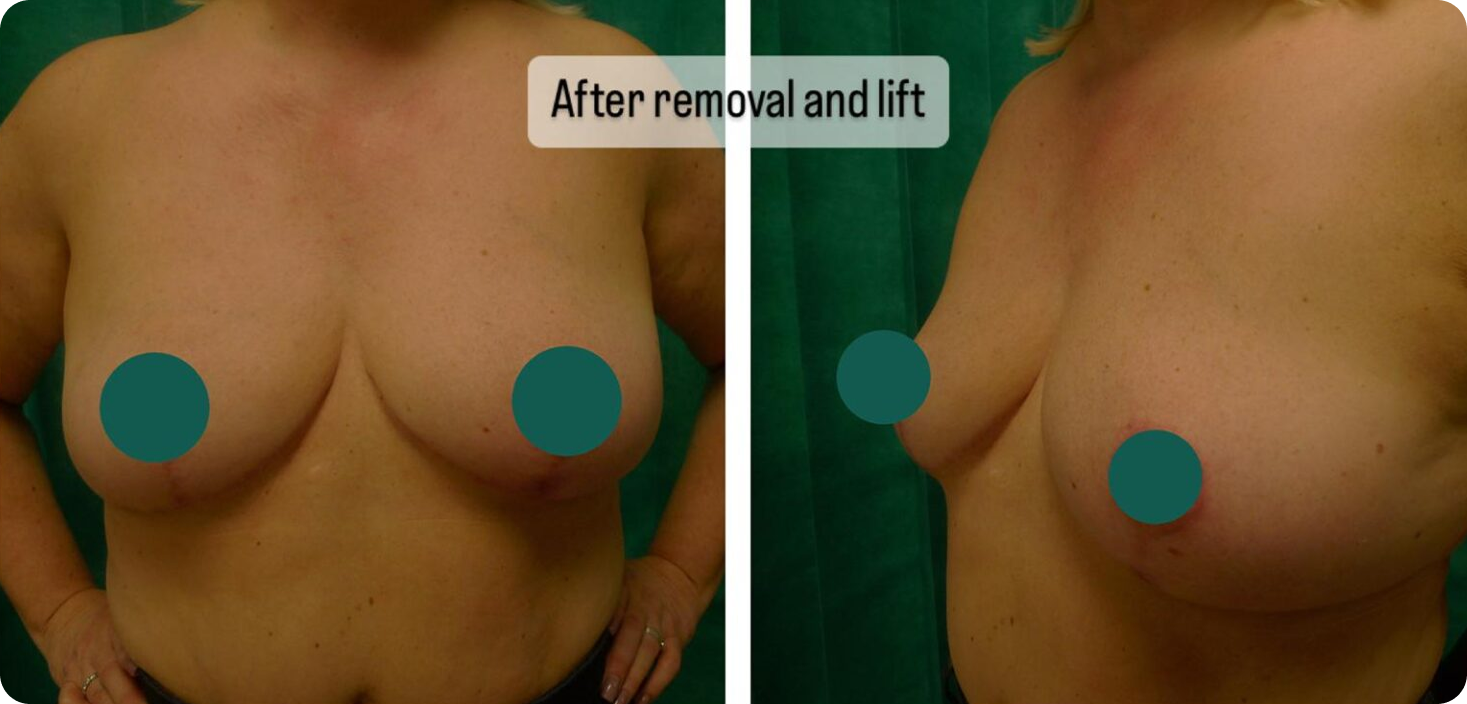
Breast Implant Removal Results
Following explantation, breasts generally appear smaller, softer and less full than when implants were present. The extent of change depends on implant size, duration of implantation, skin quality and existing breast tissue volume.
Patients who undergo simultaneous mastopexy often achieve improved breast shape, contour and nipple position compared with implant removal alone. For those seeking modest volume restoration without new implants, lipomodelling may be considered.
Patient Suitability
Breast implant removal may be suitable for patients who:
- No longer want breast implants
- Have developed capsular contracture
- Have experienced implant rupture
- Are concerned about implant-related symptoms
- Wish to reduce breast size
- Have breast sagging following augmentation
- Prefer a more natural breast appearance
- Understand the likely cosmetic changes following explantation
A consultation is required to determine whether implant removal alone, capsulectomy, uplift surgery or lipomodelling would provide the best outcome.


Breast Implant Removal & Exchange Surgery Costs
Price on consultation.
Recovery Timeline
Hospital Stay
Day surgery or overnight stay depending on complexity
Pain Management
Initial soreness and swelling during the first few days
Tenderness
Bruising and swelling gradually improve during the first few weeks. Scar maturation and breast softening continue over many months
Final Results
Final cosmetic outcome continues to improve over approximately 12–18 months
Breast Implant Removal FAQ
Common reasons include cosmetic changes, capsular contracture, implant rupture, lifestyle changes, health concerns and a desire for a more natural appearance.
Breasts often appear smaller, flatter and less full. Breast uplift surgery may help restore shape and nipple position.
It involves removing the implant and surrounding capsule together as one unit, usually where there is a specific clinical indication.
Not necessarily. Complete removal may not be safe or appropriate in all circumstances.
Yes. Mastopexy and, in selected cases, lipomodelling can improve shape following implant removal.
Yes. Some patients choose implant exchange rather than permanent explantation.
Not necessarily, but implants are not lifetime devices and should be monitored regularly.
Many patients benefit from mastopexy if implants have stretched the breast skin or caused sagging.
Most patients experience temporary discomfort, with recovery depending on the complexity of surgery and whether capsulectomy or uplift procedures are performed.